Functional occlusion. Functional occlusion: Treatment with a scientific approach
P.E. Dawson
from temporomandibular joint to smile planningIN modern world A dentist of any specialization must have basic knowledge of gnathology. Unfortunately, until now for most of our Russian colleagues this science is full of secrets and mysteries. Many are put off by the imaginary complexity, others by the imaginary controversy and the feeling of multiplicity of gnathological “concepts”, which at first glance contradict each other. However, the basis and starting point for the treatment of “gnathological” patients has always been, is and will be the temporomandibular joint.
In 120 normal non-orthodontic cases there were no rotations and no interdental spaces. The occlusal plane was not uniform throughout the specimen, but appeared within a clear and limited range of variation that clearly assumed a differential attribute.
Several intermediate conclusions were reached, and six characteristics were formulated in general outline. However, contribution to the general bank of information was necessary for many of the most qualified orthodontists at national meetings. The mesioeducational drop of the first permanent maxillary monocrystal falls into the groove between the mesial and central projection of the first permanent mandibular molar. The distal surface of the disobuccal tip of the maxillary first permanent molar contacts and is occluded by the mesial surface of the mesiobuccal tip of the second permanent lower molar. The canines and premolars have a buccal-parabolic relationship and a comminuted fossa on the tongue. In non-orthodontic models, it is systematically demonstrated that the distal surface of the dipovuccal tip of the persistent first permanent molar is overlapped by the mesial surface of the mesiobuccal tip of the permanent lower second molar.
In this book, Professor P. Dawson set himself the task of explaining in simple language something that experts sometimes unwittingly hide from their colleagues, shrouding them in a veil of secrecy and “secret knowledge.” Based on clear and understandable guidelines, scientific data, common sense and not forgetting to rely on the experience of both American and European occlusion specialists, the author reveals the secrets of success of his many years of practice. At the same time, he does not neglect, but also does not abuse, important explanations and theoretical basis.
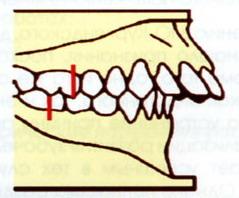
Therefore, the adequacy of the traditional description of normal molar relationships should be questioned. In Fig. Figure 1 shows how it is possible for the mesiobuccal edge of a persistent permanent molar to overlap in the groove between the mesial and central edge of the first permanent lower molar and despite an incorrect occlusion situation. The closer the distal surface of the distobuccal tip of the first permanent maxillary monocrystal is to the mesial surface of the mesiobuccal tip of the second permanent lower molar, the greater the likelihood of obtaining normal occlusion.
The author’s vast experience, critical, scientific approach, presented in a concise, accessible and clear form, which does not exclude the presence of clear recipes, ready for immediate implementation in clinical practice - distinctive features style of this book. This publication will take its rightful place in the library of every dentist, as a fundamental textbook. For some, it will become a desktop device, due to the huge number of small ideas and techniques that make the life of a practicing doctor easier.
Crown angle: mesiodistal "tip"
Figure 4 shows the molar relationship found without exception in 120 non-orthodontic models, that is, the distal surface of the upper permanent first molar contacts the mesial surface of the second permanent lower molar. It does not refer to the main axis of the entire tooth, but to the angular axis of the main axis of the crown, which in all teeth is considered the central lobe of development. In molars, the major axis of the crown is identified by the vertical groove of the buccal surface of the crown.
The gingival portion of the major axis of each crown is distal to the incisal portion. The degree of "tip" or coronal angle is the angle formed between the major axis of the crown and a line perpendicular to the occlusal plane. It is expressed in degrees: positive when the gingival portion is distal to the incisal portion and negative when the gingival portion is mesial to the incisal portion.
PREFACE
INTRODUCTION
ACKNOWLEDGMENTS
PART I. Functional Harmony
CHAPTER 1. The concept of full-fledged dentistry
CHAPTER 2. Prospects for the theory of occlusion in “everyday dentistry”
CHAPTER 3. Pathology of occlusion
CHAPTER 4. Determinants of occlusion
CHAPTER 5. Temporomandibular joint
CHAPTER 6. Chewing muscles
The angular rectangle occupies more mesiodistal space than the unglazed rectangle, this occurs in the central and lateral incisors. Normal occlusion depends on the appropriate degree of distal crown tip, especially on anterior teeth with long crowns.
The degree of "tip" of the incisors determines the amount of mesiodistal space they are going to occupy, so they have a significant impact at both the posterior level and the anterior level. The degree of coronal "tip" varies depending on the type of tooth in question.
CHAPTER 7. Central relation
CHAPTER 8. Adapted Central Position
CHAPTER 9. Determination of the central ratio
CHAPTER 10. Central Ratio Load Test
CHAPTER 11. Registration of the central ratio
CHAPTER 12. Classification of types of occlusion
CHAPTER 13. Height of occlusion
CHAPTER 14. Neutral Zone
Crown tilt
This is the angle formed between a line tangent to the location of the bracket and a line perpendicular to the occlusal plane. It is expressed in positive degrees when the gingival part is lingual to cutting edge, and negative when the gingival part is labial for the cutting edge. The inclination of all crowns is constant.
Anterior teeth: Should be sufficient to withstand the stress of the anterior teeth and to provide appropriate distal positioning of the contact points of the upper teeth relative to the lower teeth to allow proper occlusion of the posterior crowns. The inclination of the upper and lower incisors is additive and significantly affects overbite and posterior occlusion. When the incisors are very straight and low, they lose functional harmony and become overloaded.
CHAPTER 15. Functional cycle
Occlusion(Latin occludere - lock, close) is a dynamic interaction of the components of the dental system, characterized by contact of the teeth of the upper and lower jaws.
Occlusion – closure of the dentition of the upper and lower jaws (K.M. Lehmann and E. Helwig). In this position, the tubercles of the dentition are in maximum contact, that is, there is uniform bilateral contact of the tubercles and grooves.
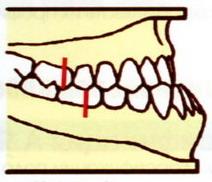
In figure a, the crowns of the upper back teeth move out of their correct position when the crowns of the front teeth are not inclined enough. Contact points move distally as the positive inclination of the crowns of the upper anterior teeth increases. Even when the upper posterior teeth are in correct occlusion with the lower inferior position, there will be unwanted gaps between the anterior and posterior teeth, as shown in Figure 7.
These spaces are often incorrectly attributed to discrepancies in tooth size in treated cases. Posterior anal teeth: The coronal inclination pattern of the maxillary posterior teeth is uniform in non-orthodontic models. There is a lingual inclination of the dental crowns, constant and similar from the canines to the second premolars, and slightly more negative in the first and second molars.
Interocclusal space– this is the distance between the resting height and the intertubercular position.
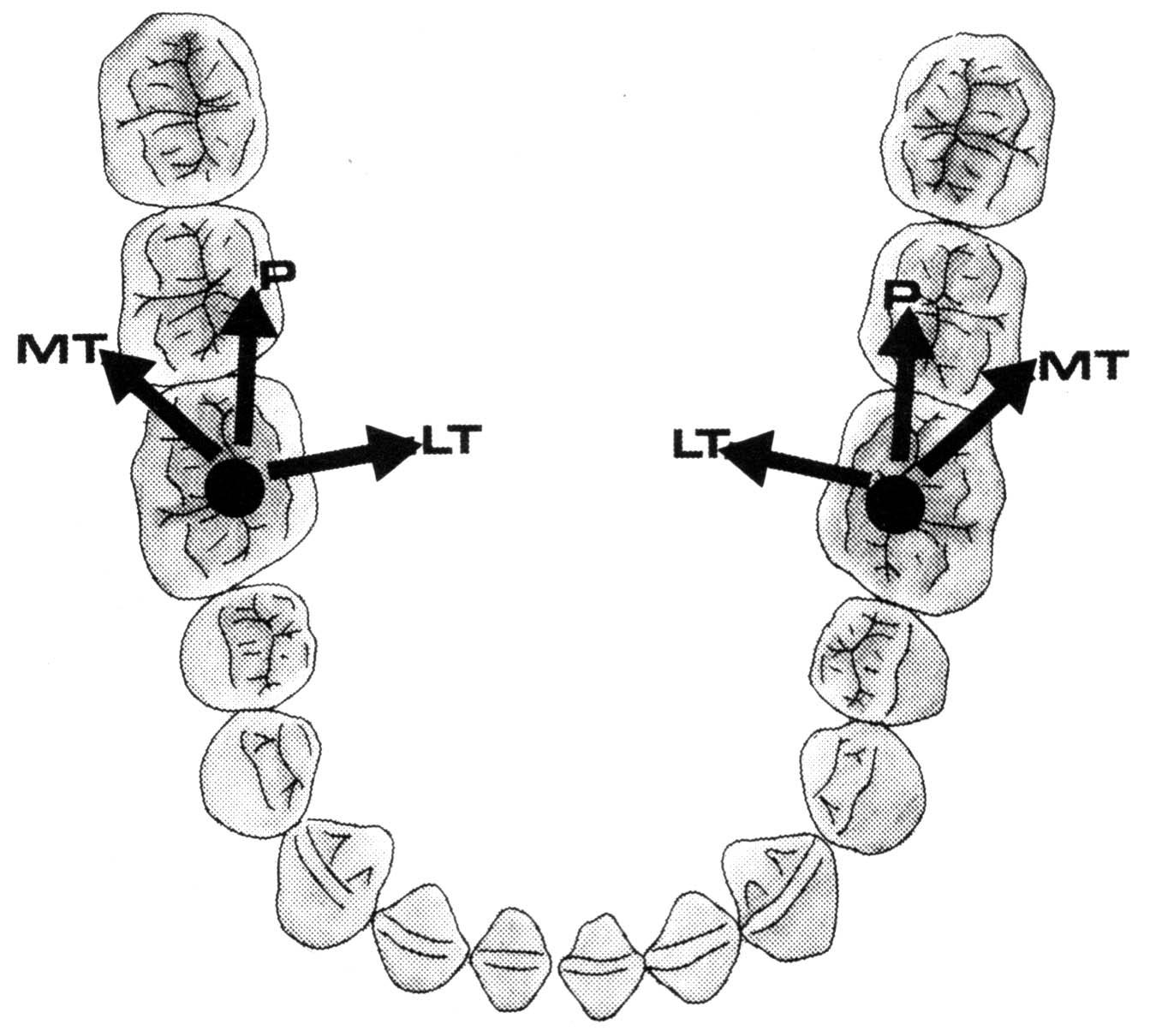
Occlusal compass - schematic representation of the occlusal movements of the cusps of the teeth from the intercuspal contact in the sagittal and transversal planes (Fig. 10).
Posteroid teeth: The pattern of coronal inclination of the mandibular posterior teeth is also uniform in non-orthodontic models. The lingual inclination of dental crowns gradually increases from the canines to the second molars. Clinical application of the second and third occlusal keys.
"Tip and Torque": When the anterior part of the rectangular wire arch is linearly twisted, a proportional amount of mesial tip of the anterior teeth crowns occurs. Let's take the example of a rectangular wire bow with four 90° welded wires that represent the upper central incisors. We see how, by twisting the wire linguistically, the vertical wires begin to converge until they become the spokes of a wheel when the wire is twisted linguistically to 90°.
Rice. 10. Occlusal compass
Occlusion can be dynamic or static.
Statistical occlusion – jaw contact in one specific position.
Dynamic occlusion – jaw contact during sliding movements.
Disocclusion – lack of contact between antagonist teeth.
Functional occlusion – dynamic contacts of the dentition in the central, lateral and anterior occlusions are the result of the integrated function of all parts of the dental system (masticatory apparatus).
Since the average distal tip for central incisors is 5°, it would be necessary to give a 10° tip distal to the arch to compensate for the mesial effect and achieve the correct coronal angulation. This mechanical problem can be easily solved if the tip and torque are interpreted in brackets rather than in the arc.
Rotation: no rotation
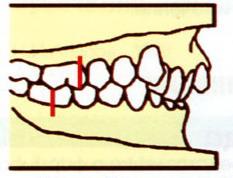
The teeth must be free from unwanted rotation because, for example, the rotation of a molar takes up more space than usual, creating an unsuitable situation for normal occlusion. In Figure 10, in this overlap we see how the rotating molar occupies the larger mesiodistal space.
Central occlusion – multiple fissure-tubercle contacts of the dentition with the central position of the heads of the temporomandibular joint in the articular fossae.
Habitual occlusion – final physiological closure of the teeth of the upper and lower jaws.
Central ratio - this is the relationship of the lower jaw in which the condyles occupy an anterosuperior position and are in contact with the central part of the articular disc located opposite the articular tubercle.
In non-orthodontic patients, without exception, there are no point-to-point gaps between the teeth. People who have true tooth size discrepancies have a particular problem, these large discrepancies should be treated with jackets or crowns, but in the absence of such anomalies, contact points should exist and be well corrected.
Although not all patients had a flat occlusal plan, Andrews believed that this situation should be a treatment target as a form of overcorrection. Even after growth, the lower molars move forward, producing the same result. If the anterior teeth can be supported until growth stops and the third molar threat has been removed by eruption or extraction, then everything should be stable, assuming the treatment was correct.
Central jaw ratio – mutual arrangement jaws in three mutually perpendicular planes.
Centric occlusion - a term that combines centric occlusion, centric sliding and posterior contact position of the teeth in the centric relation of the jaws.
Eccentric occlusion – occlusal contacts of teeth in frontal and lateral occlusions during chewing movements of the lower jaw.
Before maturation and extraction of third molars, anterior teeth should not be left except in cases where muscle control cannot be achieved during treatment and in cases where there are abnormal environmental and hereditary factors. Intercussion of teeth is best when the occlusal plane is relatively flat. There is a tendency for the occlusal plane to deepen after treatment for the reasons stated above.
It seems reasonable to treat the occlusal plane until it is somewhat flat or inverted to recognize this tendency. In many cases, it is necessary for the second permanent molars to be filled to provide an effective base for alignment of the upper and lower occlusal planes.
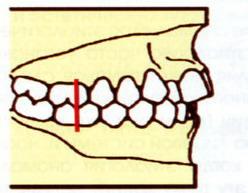
The Angle occlusion key is the upper first permanent molar. Angle identified three classes of relationship of the first permanent molars.
The remaining upper teeth, anterior and posterior to the first premolar, progress by mistake. The absence of one or more of the six results is proportional to less normal occlusion. Of course, one can observe and find models that have disadvantages, such as the need for adequate contacts, but there are dental, non-orthodontic problems. Sometimes there are intermediate weighting solutions and this poses a real challenge to the orthodontist's professional judgment.
As responsible professionals, we are here to try to achieve maximum benefit for our patients. We do not have best examples, to imitate the best of nature, and in the absence of an anomaly beyond our control, why should it be accepted?
A -IClass; b -IIClass-Isubclass; V -IIClass-IIsubclass; G -IIIClass.
Rice. eleven. Angle's classification.
In class I, there is correct fissure-tubercle contact of the lateral teeth, when the mesiobuccal cusp of the upper first permanent molar is in the anterior intercuspal groove of the lower first permanent molar. It is characterized by normal closure of the molars in the sagittal plane. All changes occur in front of the first molars (Fig. 11 a).
Satisfactory orthodontic treatment involves many disciplines, not all of which are always under our control. There are acceptable compromise treatments when patient cooperation and inheritance are required. It should not be taken unless there are any restrictions on treatment.
Since nature's non-orthodontic models provide beautiful and uniform guidelines, it seems that we should, if possible, allow these guidelines to be our measures for satisfactory orthodontic treatment. The goal of following the six keys of normal occlusion is to achieve the desired final occlusion.
In class II, there is a posterior position of the lower first permanent molar relative to the upper one. The mesiobuccal cusp of the maxillary first molar is located anterior to the intercuspal groove of the mandibular first molar.
Engle divides this class into two subclasses. For subclass I, protrusion of the upper front teeth is typical, and for subclass II, retrusion is typical. Characteristic of distal occlusion (Fig. 11 b).
Six keys to normal occlusion. Applied Operative Dentistry Introduction The term occlusion comes from the Latin occlusion, which can be defined as the act of closing or closing. Esch and Ramfjord In dentistry, this concept extends to the functional relationship between teeth and other components of the dental system. Occlusion The occlusal relationship between the maxillary and mandibular arch occurs through dental contacts on the surfaces of opposing teeth. Dental contacts, in harmony, provide occlusal stability of the archwire. Concepts in Occlusion Central occlusion It is the maximum intercussion between the arches. Also called maximal habitual intercussion or central occlusion. Central relationship It is the most anterior superior position of the condyle in the Glenoid cavity. Dislocations When making occlusal adjustments, we must also consider ideal patterns of maladaptation. Working side The side on which the jaw moves. Side of rotation Contrary to where the jaw moves. Defect as a group Partial functional defect of the group In addition to the dog, the premolars are trolled. Desocclusion in general group function Premolars and molars are affected in addition to the dog. Clinical stages of occlusal correction. Intermaxial marking with carbon paper in dynamics. Previous guides and back insulation. Wear off excess carbon with spherical diamond drills. Regularization of worn areas using 30-blade conical burr or low granulation diamonds. Occlusion is a feminine noun in Portuguese and means the act or action of closing, preventing natural flow with purposeful blocking or closing.
In class III, there is an anterior position of the lower first permanent molar relative to the upper one. The mesiobuccal cusp of the lower molar is set opposite the cusp of the second upper premolar or even more mesial. Characteristic of mesial occlusion (Fig. 11c).
Lawrence Andrews described ideal occlusion.
 (1 ratings, on average: 5,00 out of 5)
(1 ratings, on average: 5,00 out of 5)